Short answer: Semaglutide and tirzepatide are both prescription, once-weekly injectable medications used for weight management, but they are not identical. Tirzepatide acts on two gut-hormone receptors (GIP and GLP-1) while semaglutide acts on one (GLP-1), and in the first head-to-head trial comparing them — SURMOUNT-5, published in the New England Journal of Medicine in 2025 — tirzepatide produced greater average weight loss. That does not automatically make it the right choice for you. Semaglutide remains highly effective, has a longer real-world track record, and the better option depends on your medical history, tolerance, goals, and cost — a decision that belongs with a physician, not a search result.
Semaglutide vs tirzepatide at a glance
| Semaglutide | Tirzepatide | |
|---|---|---|
| Drug class | GLP-1 receptor agonist (single-pathway) | Dual GIP + GLP-1 receptor agonist |
| Common brand names | Ozempic, Wegovy, Rybelsus (oral) | Mounjaro, Zepbound |
| How it’s taken | Once-weekly injection (or daily oral tablet) | Once-weekly injection |
| Average weight loss in trials | ~15% of body weight (STEP program, 68 weeks) | ~20–25% of body weight (SURMOUNT program, 72–88 weeks) |
| Head-to-head result (SURMOUNT-5) | ~13.7% at 72 weeks | ~20.2% at 72 weeks |
| Most common side effects | Nausea, abdominal pain, heartburn, diarrhea or constipation (both) | |
| Boxed warning | Risk of thyroid C-cell tumors; contraindicated with a personal/family history of medullary thyroid carcinoma or MEN 2 (both) | |
| At Robertson Wellness (compounded) | $800/month | $925/month |
Trial percentages describe averages across study populations under controlled conditions; your own result will depend on dose, adherence, nutrition, activity, and individual biology. Numbers are a starting point for a conversation, not a promise.
What are semaglutide and tirzepatide?
Both drugs belong to a family of medications that mimic hormones your gut naturally releases after you eat. Semaglutide is a GLP-1 (glucagon-like peptide-1) receptor agonist, sold under the brand names Ozempic and Wegovy as an injection and Rybelsus as a daily tablet. Tirzepatide is a newer, dual-acting molecule — it engages both the GLP-1 receptor and a second one, GIP (glucose-dependent insulinotropic polypeptide) — and is sold as Mounjaro and Zepbound. When people compare “Ozempic vs Mounjaro” or “Wegovy vs Zepbound,” they are really comparing semaglutide vs tirzepatide.
Both are prescription medications that must be prescribed and monitored by a licensed provider. They are tools within a broader medical weight loss program that also includes nutrition, body-composition testing, and ongoing clinical supervision — not standalone shortcuts.
How do they work? (mechanism of action)
Semaglutide activates the GLP-1 receptor, which does three main things: it slows how quickly your stomach empties, signals fullness to the appetite centers of your brain, and helps regulate blood-sugar and insulin response. In plain terms, it makes you feel satisfied sooner and stay full longer, so you naturally eat less.
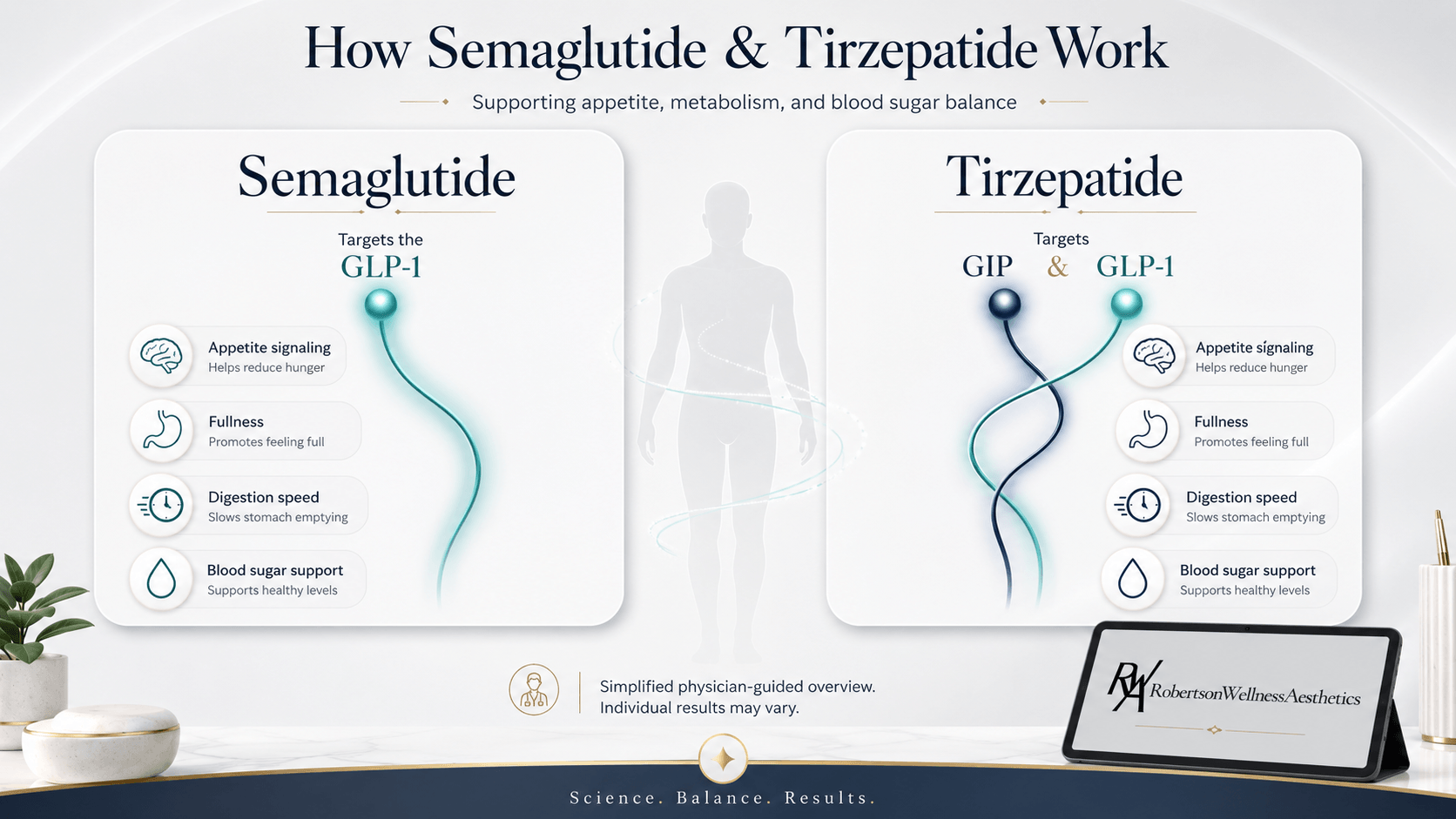
Tirzepatide does everything semaglutide does through the GLP-1 pathway, then adds a second signal through the GIP receptor. GIP is thought to further improve how the body handles blood sugar and fat and may enhance the appetite-suppressing effect while helping to temper nausea. This “dual agonist” design — hitting two complementary gut-hormone pathways at once — is the leading explanation for why tirzepatide tends to produce greater weight loss on average. The dual mechanism is described in the pivotal SURMOUNT-1 trial (Jastreboff et al., New England Journal of Medicine, 2022).
Which one causes more weight loss?
For most patients in clinical trials, tirzepatide produced more weight loss than semaglutide — and in 2025 that comparison stopped being indirect. SURMOUNT-5 (Aronne et al., New England Journal of Medicine, 2025) was the first randomized head-to-head trial to put the two drugs against each other in the same study. Among 751 adults with obesity but without type 2 diabetes, treated for 72 weeks at maximum tolerated doses, participants on tirzepatide lost about 20.2% of their body weight versus about 13.7% on semaglutide — roughly 50% more relative weight loss. Tirzepatide also showed greater average improvements in waist circumference and several cardiometabolic markers.
This is meaningful, but three caveats matter. First, these are averages: some people lose more on semaglutide than the average person does on tirzepatide. Second, “more weight loss” is not the only goal — tolerability, safety, cost, and whether you can stay on the medication long-term all shape the real-world outcome. Third, the most effective medication is the one a patient can take consistently and safely, which is an individual determination. Effectiveness on paper and the right fit for you are not always the same thing.
Side effects and safety: how do they compare?
Semaglutide and tirzepatide share a very similar safety profile because they work through overlapping pathways. The most common side effects for both are gastrointestinal: nausea, abdominal pain, heartburn, and diarrhea or constipation. These are usually most noticeable when starting the medication or increasing the dose, and they often ease over time. Slow, gradual dose escalation (titration) and simple measures like hydration and dietary adjustments are the standard ways to manage them; persistent or severe symptoms should always be reported to your provider. A comparative safety review (Pharmacological Research, 2025) found the two medications broadly comparable in their side-effect patterns, with GI effects dominating for both.
Both medications also carry the same boxed warning — the FDA’s most serious — regarding a risk of thyroid C-cell tumors observed in rodent studies. Because of this, both are contraindicated in anyone with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). They are also generally not appropriate for people with a history of pancreatitis, and are not used during pregnancy. Rare but serious risks reported with GLP-1-based medications include pancreatitis, gallbladder problems, and serious allergic reactions. This is precisely why a thorough medical evaluation comes before any prescription — screening for these conditions is part of responsible care.
How much do they cost?
Cost is often the deciding factor in the real world. At Robertson Wellness and Aesthetics, the medical weight loss program is priced at $800 per month for semaglutide and $925 per month for tirzepatide, with a $450 initial consultation that can be waived with the purchase of a package. Programs run on a three-month minimum, reflecting how these medications are intended to be used — titrated and monitored over time, not started and stopped abruptly.
A note on formulation and FDA status, because patients deserve the full picture: the compounded semaglutide and tirzepatide offered in many clinic weight-loss programs are prepared by compounding pharmacies and are not FDA-approved products, unlike the branded versions (Wegovy, Zepbound). The FDA does not verify the safety or effectiveness of compounded drugs. What makes compounded therapy defensible is the clinical framework around it: licensed physician oversight, sourcing from compliant pharmacies, and individualized dosing and monitoring — the same standard that governs the rest of our care, from peptide therapy to hormone optimization.
✓ No contracts
★★★★★
5.0 on Yelp · 35+ reviews
Not sure which GLP-1 is right for you?
The choice between semaglutide and tirzepatide is a clinical one. Our Beverly Hills physicians review
your health history, goals, and labs, then recommend the medication and dose that fit you —
prescribed and monitored under medical supervision, with concierge in-home and hotel visits available.
*$450 initial consultation can be waived with the purchase of a package. These statements have not been
evaluated by the FDA. Semaglutide and tirzepatide are prescribed only after a medical evaluation by a
licensed provider, are not appropriate for everyone, and individual results vary.
Which is right for you? A decision framework
There is no universally “better” GLP-1 medication — only the better fit for a given person. In a consultation, a physician weighs factors like these:
- Your weight-loss goal and starting point. Patients with more weight to lose, or who have plateaued on semaglutide, may be candidates for tirzepatide’s greater average efficacy.
- Tolerability. Some people tolerate one medication’s side effects better than the other. How your body responds during titration is real data that guides the plan.
- Medical history. Thyroid history, pancreatitis, gallbladder issues, diabetes, and current medications all shape whether either drug is appropriate.
- Cost and sustainability. The best medication is one you can stay on. Monthly cost and long-term plans matter as much as trial percentages.
- Preferences. Injection vs oral options, dosing schedule, and how the medication fits your life all factor in.
For many high-consideration patients in Beverly Hills, Bel Air, and West Hollywood — as well as visiting executives and hotel guests near Cedars-Sinai and Rodeo Drive — GLP-1 therapy is one piece of a broader wellness strategy that may also include NAD+ IV therapy or, for men, physician-supervised TRT. Coordinating these under one clinical team is part of how care is personalized here.
Can you switch between them?
Yes — many patients start on one medication and transition to the other under medical supervision, whether because of side-effect tolerance, a weight-loss plateau, cost, or availability. Switching is a clinical decision that involves appropriate dose matching and re-titration; it should never be done by self-adjusting or sourcing medication outside a supervised program. If your current approach isn’t working the way you hoped, that is a conversation to have with your provider, not a reason to stop care.
Medical Disclaimer
These statements have not been evaluated by the Food and Drug Administration. This article is for educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. Semaglutide and tirzepatide are prescription medications that must be prescribed and supervised by a licensed healthcare provider following an individual medical evaluation. They are not appropriate for everyone, carry a boxed warning regarding thyroid C-cell tumors, and are contraindicated in patients with a personal or family history of medullary thyroid carcinoma or MEN 2. Compounded formulations are not FDA-approved, and the FDA does not verify the safety or effectiveness of compounded drugs. Individual results may vary. Always consult a qualified healthcare provider before beginning any new treatment.
Frequently asked questions
Is tirzepatide or semaglutide better for weight loss?
In the SURMOUNT-5 head-to-head trial, tirzepatide produced greater average weight loss than semaglutide (about 20.2% vs 13.7% of body weight at 72 weeks). On average, tirzepatide tends to be more effective, but semaglutide is also highly effective, and the “better” option for any individual depends on medical history, tolerance, cost, and goals. That determination is made with a physician.
Which is safer, semaglutide or tirzepatide?
Both have very similar safety profiles because they work through overlapping pathways. The most common side effects for each are gastrointestinal (nausea, abdominal discomfort, changes in bowel habits), and both carry the same boxed warning about thyroid C-cell tumors and the same key contraindications. Neither is categorically “safer” — safety depends on the individual patient, proper screening, correct dosing, and ongoing medical supervision.
Are semaglutide and tirzepatide the same as Ozempic and Mounjaro?
Semaglutide is the active ingredient in Ozempic, Wegovy, and Rybelsus. Tirzepatide is the active ingredient in Mounjaro and Zepbound. So “semaglutide vs tirzepatide” is the same comparison as “Ozempic/Wegovy vs Mounjaro/Zepbound” — just by generic name rather than brand.
How quickly will I see results?
Most people begin to notice changes within a few weeks to a couple of months, with weight loss typically in the range of 1 to 3 pounds per week alongside proper lifestyle changes. The pace varies with dose, adherence, nutrition, and individual biology, and both medications are titrated gradually rather than started at full dose. Results are not guaranteed and vary between individuals.
Do I need a prescription, and can I get these at a medical spa?
Yes, both require a prescription from a licensed provider following a medical evaluation. At Robertson Wellness and Aesthetics, they are offered within a physician-supervised weight management program that includes screening, individualized dosing, and follow-up — not sold over the counter. You can meet the clinical team and begin with a consultation.
Talk to a physician before you choose
If you’re weighing semaglutide against tirzepatide, the most useful next step isn’t picking a winner from an article — it’s a consultation that matches the medication to your body, history, and goals. Robertson Wellness and Aesthetics offers physician-supervised GLP-1 weight management in Beverly Hills, with in-clinic and concierge options. Book a consultation to find out which approach fits you.