The short answer: Growth-hormone peptides such as CJC-1295, ipamorelin, and sermorelin are short chains of amino acids that signal a man’s own pituitary gland to release more of its own growth hormone, rather than injecting synthetic growth hormone from outside. In men’s hormone optimization they are used mainly to support recovery, sleep quality, body composition, and tissue repair — the areas tied to the growth-hormone/IGF-1 axis that tends to decline with age. They are prescribed off-label, only after a physician evaluation and bloodwork, and are not appropriate for everyone.
What are growth-hormone peptides?
Growth-hormone peptides — often called growth-hormone secretagogues — are short amino-acid chains that prompt the pituitary gland to secrete the body’s own growth hormone (GH). This is a meaningfully different approach from injecting recombinant human growth hormone (rHGH), which floods the body with hormone from an outside source. Because secretagogues work through your own pituitary, they tend to preserve the natural, pulse-like rhythm of GH release and keep output within physiologic ranges (neuroendocrine regulation of growth-hormone secretion, published in PubMed Central).
Interest in these peptides rises after 40 for a simple reason: growth-hormone output and its downstream marker, insulin-like growth factor 1 (IGF-1), decline gradually with age, and many men notice it as slower recovery, lighter or less restorative sleep, and a harder time holding lean muscle. Peptides are one physician-supervised option explored to support that axis — distinct from, and sometimes complementary to, testosterone-focused care. If your primary concern is libido, mood, or diagnosed low testosterone, that is a different system; see our guide to low testosterone symptoms in men and how TRT and peptides differ.
How do CJC-1295, ipamorelin, and sermorelin work? (mechanism of action)
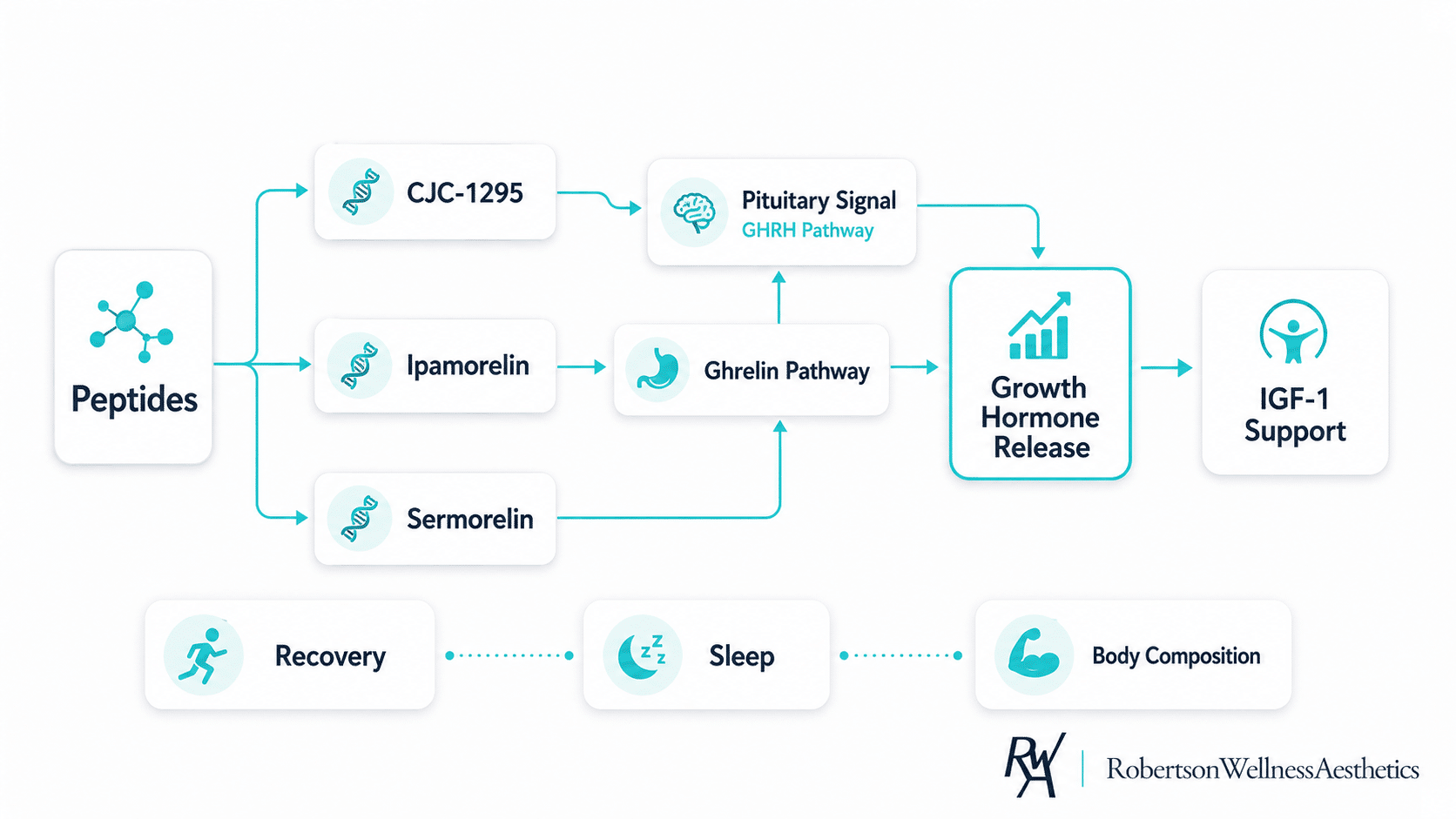
All three belong to the growth-hormone-secretagogue family, but they act through two different doors on the pituitary, which is why they are often discussed together.
Sermorelin and CJC-1295: GHRH analogs
Normally, the hypothalamus releases growth-hormone-releasing hormone (GHRH) to tell the pituitary’s somatotroph cells to make and release GH. Sermorelin is a synthetic fragment corresponding to the first 29 amino acids of human GHRH — the GHRH(1-29) segment that retains essentially the full biological activity of the natural hormone — so it binds GHRH receptors and stimulates GH synthesis and release, then clears quickly from the blood (Prakash & Goa, review of sermorelin, PubMed). CJC-1295 is a longer-acting analog of GHRH engineered to resist breakdown; in a placebo-controlled trial in healthy adults, a single subcutaneous dose produced dose-dependent increases in GH of roughly 2- to 10-fold and in IGF-1 of about 1.5- to 3-fold, with effects lasting several days (Teichman et al., Journal of Clinical Endocrinology & Metabolism, 2006). In plain terms: both mimic the body’s own “release GH” signal, with sermorelin acting briefly and CJC-1295 extending that signal.
Ipamorelin: a selective ghrelin-receptor peptide
Ipamorelin works through a separate pathway. It is a pentapeptide that acts on the ghrelin (GHS-R1a) receptor, and it was characterized as the first selective growth-hormone secretagogue — meaning it prompts GH release with little effect on other hormones such as cortisol and prolactin in preclinical work (Raun et al., “Ipamorelin, the first selective growth hormone secretagogue,” European Journal of Endocrinology). Because CJC-1295 pushes the GHRH door and ipamorelin pushes the ghrelin door, clinicians often pair them (commonly “CJC-1295 / ipamorelin”) so the two complementary signals can amplify GH release while still following the body’s pulse-like pattern.
The practical marker of all this activity is IGF-1. In a study of hypogonadal men, growth-hormone-secretagogue treatment raised serum IGF-1, the downstream signal of GH action (Sigalos et al., growth-hormone secretagogue treatment in men, American Journal of Men’s Health).
What peptides support for men over 40
Men explore growth-hormone peptides for goals tied to the GH/IGF-1 axis rather than the testosterone axis. Framed honestly as areas the therapy may support — not guaranteed outcomes — those typically include:
- Recovery and tissue repair — supporting the body’s repair processes after training or physical demand.
- Sleep quality — GH secretion is closely linked to deep sleep, and better sleep is a frequently reported goal.
- Body composition — supporting lean mass and fat metabolism as part of a broader program of training and nutrition, not in place of it.
- Age-related decline in GH output — providing a signaling approach for men who prefer stimulating their own production over introducing an outside hormone.
What peptides are not is a shortcut. Changes unfold over weeks to months, vary considerably between individuals, and depend heavily on sleep, nutrition, training, and adherence. No responsible clinic promises a fixed result by a fixed date.
✓ No contracts
★★★★★
5.0 on Yelp · 35+ reviews
Curious whether peptide therapy fits your goals?
Peptide protocols aren’t one-size-fits-all. Our Beverly Hills physicians build your plan after a
consultation and bloodwork — matched to your labs, goals, and medical history, and sourced from
compliant compounding pharmacies under medical supervision.
These statements have not been evaluated by the FDA. Treatment is not intended to diagnose, treat,
cure or prevent any disease. Peptide therapy is prescribed only after a medical consultation and
evaluation by a licensed provider, and is not appropriate for everyone.
Who is peptide therapy for — and who is it not for?
Peptides are generally considered for men over 40 whose goals center on recovery, sleep, and body composition, who have realistic expectations, and who want a physician-supervised, signaling-based approach. Candidacy is a clinical decision that depends on your goals, baseline labs, and full medical history — which is why a consultation and comprehensive lab testing and biomarker analysis come first, not after.
Just as important is who peptides are not for. They are not a treatment for diagnosed low testosterone — that is the androgen axis, and it calls for a different evaluation and, when appropriate, physician-supervised TRT. They are generally not appropriate for anyone with an active or history of cancer, and they warrant caution in men with diabetes or blood-sugar concerns, given growth hormone’s effect on insulin sensitivity. Anyone considering peptides should disclose their full medical history and current medications so a provider can assess fit and safety.
What to expect during peptide therapy at RWA
At Robertson Wellness and Aesthetics, peptide therapy begins with a consultation and bloodwork rather than a protocol pulled off a shelf. A physician reviews your goals, symptoms, and labs, determines whether a growth-hormone-secretagogue approach fits, and — if it does — designs a plan with appropriate dosing and monitoring. Growth-hormone peptides are typically given as small subcutaneous injections, often in the evening to align with the body’s natural nighttime GH pulse, and progress is re-checked with follow-up labs over time.
Two things define legitimate care here. First, sourcing: peptides should come from compliant compounding pharmacies under physician supervision, not from online sellers of research chemicals of unknown potency or sterility. Second, integration: for many high-consideration patients in Beverly Hills, Bel Air, and West Hollywood — as well as visiting executives and hotel guests — peptide therapy sits alongside other longevity-focused care, from NAD+ IV therapy to hormone optimization, coordinated so the pieces work together. Concierge in-home and hotel visits are available for patients who prefer treatment on their own schedule.
Side effects, safety, and FDA/regulatory status
Reported side effects of growth-hormone peptides can include injection-site reactions (redness, itching, or swelling), water retention, joint discomfort, tingling or numbness, headache, and changes in blood-sugar handling. Long-term safety data in healthy aging men is more limited than the decades of evidence behind testosterone therapy, which is one reason physician oversight and periodic labs matter.
The regulatory picture deserves plain language, because patients are often given a rosier version than the facts support. Most growth-hormone peptides marketed for anti-aging or wellness are not FDA-approved for those uses; their use is off-label. Sermorelin was previously FDA-approved (as Geref) for pediatric growth-hormone deficiency but was discontinued for commercial reasons around 2008; it remains available today only as a compounded medication. The one GHRH analog with current FDA approval is tesamorelin (Egrifta), and only for a specific HIV-associated condition — not general anti-aging. The compounding landscape is also actively shifting: U.S. regulators have been re-evaluating which peptide substances pharmacies may compound, with formal review ongoing in 2026. For a reputable clinic, the takeaway is straightforward: peptide protocols should be physician-supervised and sourced from compliant pharmacies, and any provider who glosses over the off-label reality is not giving you the full picture.
Medical Disclaimer: These statements have not been evaluated by the Food and Drug Administration. This information is for educational purposes only and is not intended to diagnose, treat, cure, or prevent any disease. Peptide therapy is a medical treatment that must be prescribed and supervised by a licensed healthcare provider following an individual evaluation. It is not appropriate for everyone, and individual results may vary. Always consult a qualified healthcare provider before beginning any new treatment.
Frequently asked questions
What is the difference between CJC-1295 and ipamorelin?
They stimulate growth-hormone release through two different receptors. CJC-1295 is a long-acting GHRH analog that acts on the GHRH receptor to extend the “release GH” signal, while ipamorelin is a selective ghrelin-receptor peptide that triggers a more immediate GH pulse. Because the pathways are complementary, they are frequently prescribed together so the effects can reinforce one another.
Is sermorelin better than CJC-1295?
Neither is universally “better” — they differ mainly in duration. Sermorelin is a short-acting GHRH fragment that clears quickly, while CJC-1295 is engineered to last longer in the body. The right choice depends on your goals, response, and a physician’s assessment, not on a blanket ranking.
Are peptides for men safe?
When prescribed and monitored by a licensed provider, using peptides sourced from compliant pharmacies, growth-hormone peptides are generally well tolerated, with side effects such as injection-site reactions, water retention, or joint discomfort. Long-term data in healthy aging men is limited, and safety depends on the right candidate, correct dosing, and ongoing oversight — not on buying peptides online.
Do growth-hormone peptides raise testosterone?
No. CJC-1295, ipamorelin, and sermorelin act on the growth-hormone/IGF-1 axis, not the testosterone axis, so they should not be expected to correct clinically low testosterone. If your testosterone is genuinely low, testosterone replacement therapy — not peptides — is the therapy designed to address it.
How soon do peptides work?
Results typically unfold over weeks to months and vary between individuals depending on dose, adherence, sleep, nutrition, and activity. Reputable clinics set realistic expectations and re-check labs rather than promising a specific outcome by a specific date.
Talk to a physician before you decide
If you’re a man over 40 considering CJC-1295, ipamorelin, or sermorelin, the most valuable next step is a consultation and comprehensive bloodwork — not an online purchase. Robertson Wellness and Aesthetics offers physician-supervised peptide therapy in Beverly Hills, with both in-clinic and concierge options. Book a consultation to find out whether peptides fit your goals, your labs, and your health history.